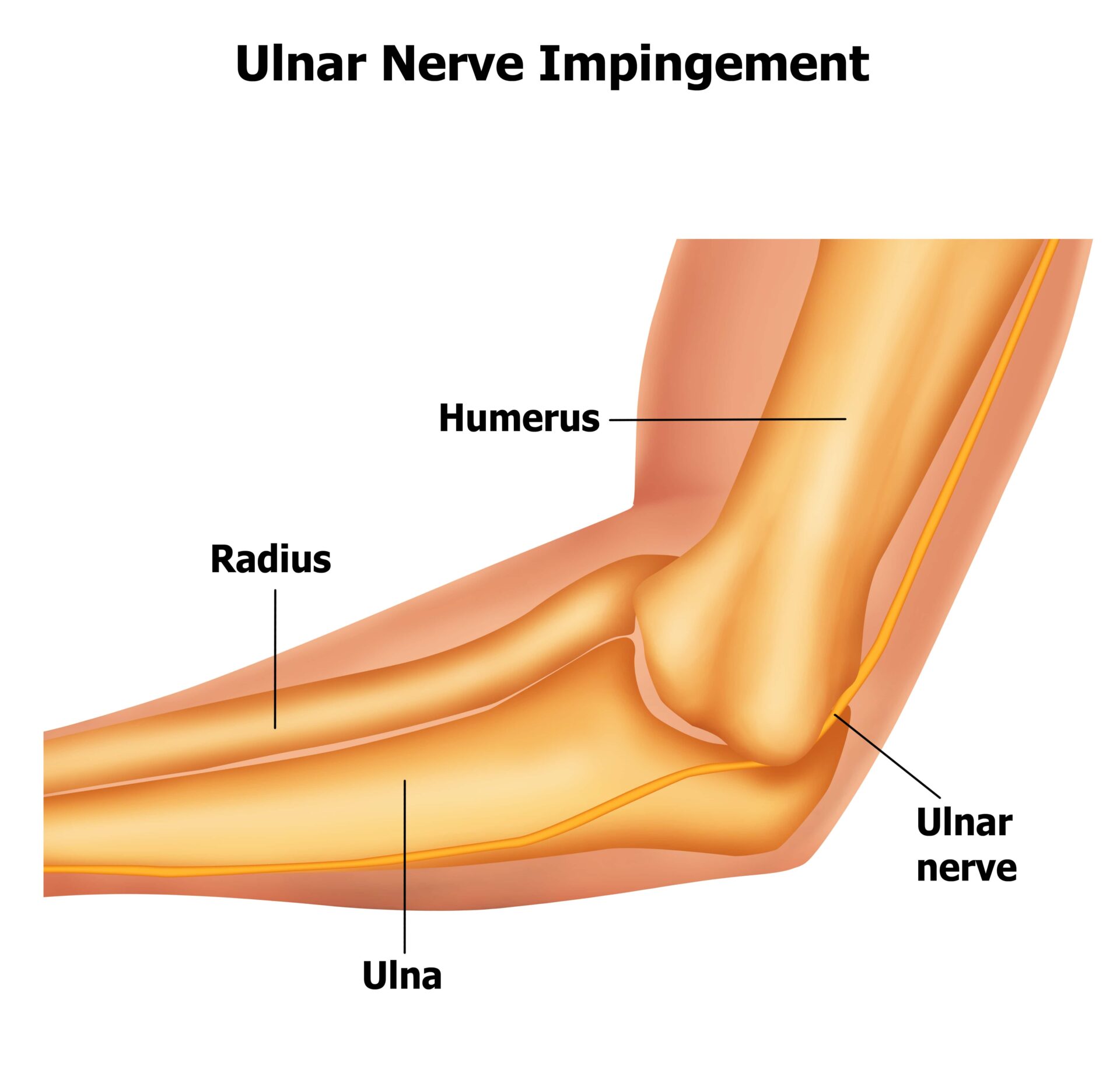
Cubital tunnel syndrome is compression or irritation of the ulnar nerve, which is located in a tunnel on the inside of the elbow. This area of the body is more commonly known as the “funny bone.” So what does the ulnar nerve do? Well, it provides sensation to the little finger and part of the ring finger, and power to most of the small muscles within the hand.

Cubital Tunnel Treatment
Book Appointment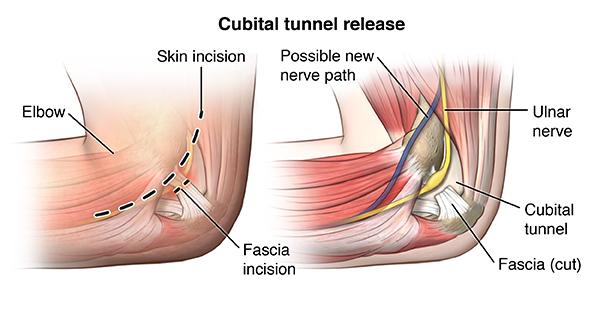
Causes
There are few known causes of cubital tunnel, but the specifics include:
- The tunnel can be narrowed by pressure from the muscle or ligaments, arthritis of the elbow joint or by an old injury however in most cases there are no obvious cause
- Pressure due to the nerve padding deteriorating, and when one leans on their arm or hand, it can press the nerve
- Stretching the elbow, or keeping it bent in a specific way for a long period of time – this can happen during periods of sleep
- Traumatic injury to the elbow and inadequate recovery
Symptoms
Early signs of cubital tunnel: intermittent numbness or tingling of the little and ring fingers.
Late signs: persistent numbness and weakness of the hand (loss of dexterity and strength).
Often the symptoms can be provoked by leaning on the elbow or holding the elbow in a bent position (e.g. on the telephone). Sleeping with the elbow habitually bent can also aggravate the symptoms.
Investigations may include x-rays of the elbow and nerve conduction studies.
Treatments
Avoid or modify any provocative activity where appropriate. These manoeuvres may be curative in early cases. For example,
- Wear a headset while using the telephone
- Avoid leaning on the inside of the elbows or wear protective pads
- Excessive bending of the elbow at night can be minimised by a folded towel wrapped around the elbow, or using an elbow splint.
Surgery to decompress the nerve is required in severe cases, or in those that do not respond to the above non-surgical treatments.
Surgery frequently improves the numbness, but its main objective is to prevent the progressive muscle weakness and wasting that tends to occur in untreated cases.
Several operations are described under general or regional anaesthetic, based on the cause of the condition. These include,
- Opening of the roof of the tunnel (decompression).
- Moving the nerve into a new location at the front of the elbow (transposition).
- Widening the tunnel by removing some of its bony floor (medial epicondylectomy).
Aftercare and Follow-Up
The operated arm should be kept dry and clean for 2 weeks while the wound heals. One week after the procedure the dressing are reduced by the practice nurse. The sutures are absorbable and the ends are removed at 2 weeks after surgery in the clinic. Normal daily activities and use of the arm is encouraged to avoid elbow stiffness.
If nerve transposition is carried out, the arm needs to remain in the sling for 2 weeks, to allow the nerve to settle down in its new location. Elbow exercises for one minute, three times a day in the first 2 weeks are required to stop the elbow from getting stiff leading to tendon and nerve adhesions. Physiotherapy will be arranged formally after 2 weeks when the wound has healed.

Driving
You should allow a period of approximately 2 weeks before driving. You will need to be collected from hospital after the operation.
Time Off Work
Your return to work will depend on your job. Light manual workers can return to duty in 2 – 3 weeks. Heavy manual workers should not exert maximal grip and excess force on the elbow for 6 weeks.
Scar Desensitisation Exercises
- Circular motion massages to the scar, using a simple moisturising cream and the palm of the opposite hand. This must be carried out for 10 minutes, at least 3 times a day.
- Rubbing the scar on different textured materials to improve skin sensitivity.
- Submerging the hand under cold and warm water to improve the temperature sensitivity.

Risks of Surgery
- Infection
- Injury to ulnar nerve and blood vessels
- Scar sensitivity (Scar desensitisation exercises after 2 weeks will help to improve scar sensitivity however this can last up to 6 months after surgery).
- Recurrence
- Failure to resolve all symptoms (If there is long-standing compression of the ulnar nerve there may be irreversible changes of numbness and/or weakness in the hand).
- Further surgery (in the event of recurrence or other complications)
- Reduced grip strength
- CRPS (chronic pain syndrome: A small percentage of patients will develop a severe reaction after hand surgery, with lifelong permanent pain and stiffness which is unresponsive to treatment.)
Outcome
The outcome depends upon the severity and period of symptoms experienced by the patient. In the mild cases, full resolution of symptoms occurs in most cases. Numbness frequently improves, though the improvement may be slow and can take up to 18 months.
Surgery generally prevents worsening of the muscle weakness, but improvements in muscle strength are often slow and incomplete. In the more severe cases, the long-term outcome in regard to nerve recovery is unpredictable.
Book an appointment
Please use this form if you are interested in booking an appointment. We do not give general medical advice over email.