
Scapholunate Ligament Tear Treatment
Book AppointmentThe wrist is a complex joint consisting of 8 small bones, connected to each other with many strong ligaments. The scapholunate ligament is an important ligament that holds the scaphoid and lunate bones together. When ruptured it can cause pain and instability in the wrist in short term and degenerative arthritis in 5-10 years.
The injury often results from a fall onto the outstretched hand or a forceful/violent twisting injury to the hand.
Symptoms of Scapholunate Ligament Tear
The symptoms of scapholunate ligament tear depend on whether the injury is acute (recent) or chronic Longstanding).
Acute injury:
- Wrist pain
- Stiffness
- Swelling
- ‘Clunking’ – this is often painful
- Loss of grip strength
Chronic injury:
- Weakness
- Clunking
- Pain after use
- Background pain (usually from secondary arthritis)
Diagnosis
Wrist tenderness is usually centred on the scapholunate ligament with some swelling in the same region. Wrist movement may be restricted, stiff and painful. The Kirk-Watson test is specific to the scapho-lunate ligament and a positive test indicates either a ligament injury or scaphoid fracture.
Investigations
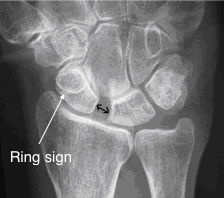
1. X-rays usually show;
- Widening of the scapholunate gap (Terry Thomas sign – named after the actor with a large gap in his front teeth)
- The ‘ring sign’ on the the scaphoid
2. MRI scan which can show the actual ligament tear and swelling
3. Wrist arthroscopy (keyhole surgery) which can allow the ligament to be visualized in real time.
Scapholunate Ligament Tear Treatments
Partial tear
Scapholunate ligament tear treatment typically involves addressing ligament sprains where one or two parts of this three-part ligament are injured, without resulting in wrist instability. In such cases, a recommended approach is immobilization in plaster for about 4-6 weeks, followed by the administration of analgesics and hand therapy. The recovery process may span up to 18 months.
Complete tear
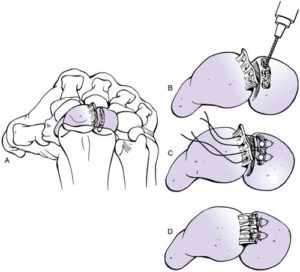
In the presence of an acute (within 8 weeks of the injury) complete ligament rupture, direct anatomical repair leads to satisfactory results. The ligament is exposed at the back of the wrist under general anaesthetic and with the use of small bone anchors the ligament repair is carried out. Wires are then inserted along with a plaster cast, to immobilize the wrist joint for 8 weeks while the ligament heals. At 8 weeks after the initial surgery the wires are removed under general anaesthetic and movement of the wrist starts with the help of the hand therapist and regular analgesia.
In the presence of a chronic (8 weeks after the injury) complete ligament rupture, scapholunate ligament tear treatment is not possible and a ligament reconstruction is recommended. Under general anaesthetic half of a tendon in front of the wrist is passed through a tunnel in scaphoid and then fixed to the lunate to close the gap between the two bones. Wires are then inserted along with a plaster cast, to immobilize the wrist joint for 8 weeks while the ligament heals. At 8 weeks after the initial surgery the wires are removed under general anaesthetic and movement of the wrist starts with the help of the hand therapist and regular analgesia.
In the presence of a chronic complete ligament rupture and established arthritis, ligament reconstruction is not possible and treatment of arthritis is recommended (please see section on wrist arthritis).
Aftercare and Follow Up
Regular follow up by hand therapists are required after the plaster and the wires have been removed. As the recovery can take a long time, one needs to remain motivated and continue with the treatment plan.
Driving
Driving will not be allowed up to 12 weeks after surgery.
Time off work
Your return to work will depend on your job. Office workers can return to duty in 2 – 3 weeks. Heavy manual activities should not be performed for 12 weeks.
Scar desensitisation exercises
- Circular motion massages to the scar, from the palm moving towards the wrist using a simple moisturising cream. This must be carried out for 10 minutes, at least 3 times a day.
- Rubbing the scar on different textured materials to improve skin sensitivity.
- Submerging the hand under the cold and warm water to improve the temperature sensitivity.

Risk of Surgery
- Infection
- Injury to superficial nerve, blood vessels and tendons
- Scar sensitivity (Scar desensitisation exercises after removal of stitches help to improve scar sensitivity however this can last up to 6 months after surgery)
- Recurrence (ligament reconstruction can stretch with time and further injury).
- Failure to resolve all symptoms (in presence of arthritis)
- Further surgery (in event of recurrence or other complications)
- Reduced grip strength
- Reduced range of wrist movements (up to 40% loss of motion)
- CRPS (chronic pain syndrome: A small percentage of patients will develop a severe reaction after hand surgery, with lifelong permanent pain and stiffness which requires extensive physiotherapy and pain medication)
Sound familiar? Get in touch
Please use this form if you are interested in booking an appointment. We do not give general medical advice over email.